

Tackling inequalities: could Covid’s legacy be a great redistribution of health?
Few events have more vividly and visibly highlighted the UK’s growing health inequalities than the COVID-19 pandemic. But could the nation’s sobering awakening actually become the catalyst for meaningful and lasting change?
Over recent decades, successive governments and initiatives have tried and largely failed to overturn the inherent health inequalities across the UK. While always felt acutely by those affected, these inequalities rarely strayed into the mainstream consciousness for long.
That all changed during the COVID-19 pandemic. The healthy got healthier and the less healthy got less healthy still, said public-health expert Professor Devi Sridhar at the Royal Society of Medicine’s ‘COVID-19: Two years on’ event in March 2022. For the first time in any meaningful way, headlines about the disproportionate impacts of deprivation, ethnicity, disability, gender and class on health outcomes were absorbed by households up and down the land. Health inequalities became front page news.
Some believe this unprecedented exposure could be the catalyst to do what other programmes have failed to do and tackle health inequalities once and for all.
It is an idea gaining increased support by the healthcare community. Respiratory registrar Dr Neeraj Shah, President of the Royal Society of Medicine Respiratory Medicine Section, said: “In the past when we’ve tried to deal with this, we haven’t had a big trigger. This is the time, when we have the momentum to deal with it.”
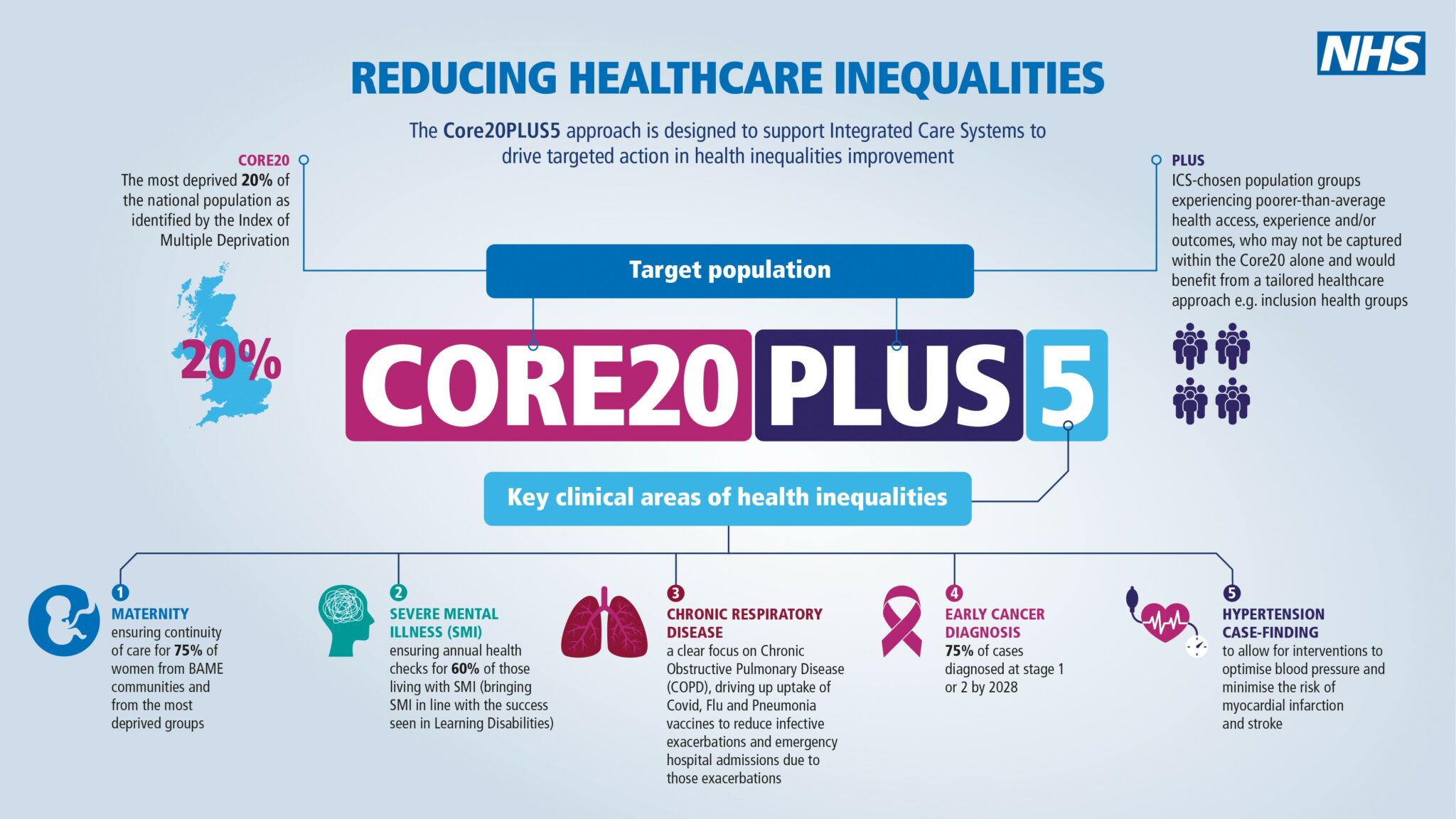
Dr Shah’s field is at the sharp end of health inequalities. Respiratory disease is the third biggest killer in the UK and it is, he said, “completely wrapped up” with socioeconomic status. It is for this reason that chronic respiratory disease is one of five clinical areas in the sights of the NHS Core20PLUS5 initiative to tackle health inequalities. By focusing energy on where inequalities are starkest, the initiative hopes to have a far bigger impact than it would if it spread resources equally across specialties and conditions.
Dr Bola Owolabi, Director - Health Inequalities at NHS England and NHS Improvement, writing in BMJ Leader in February 2022, said: “Health inequalities have been around for decades, and they certainly won’t disappear overnight. As clinicians, the impact of health inequalities on the communities we serve is something we will see throughout our careers. We need health and care leaders to be mindful of the challenge – and the opportunity they have to make a difference.”
The accumulated impact of living with chronic poor health or disability can be ruinous for individuals and families. Sussex-based Louise Ives’ son, Kieran, was diagnosed with Duchenne muscular dystrophy nearly 25 years ago. While she cares for 28-year-old Kieran “happily”, Louise said the impact on her life has been “utterly devastating”.

As Kieran has become more disabled over the years, single mother Louise has given up work, sold her house, no longer goes on holiday and will be 70 years old before she pays off her new mortgage. She loves caring for Kieran but feels that’s not the point. She said: “My life shouldn't have changed so dramatically because of one person needing some care.
“The whole system isn't set up for you to care for someone at home and be supported.”
The ‘system’, as she experiences it, sees her interacting with multiple agencies in what she describes as a “constant struggle” to get Kieran’s needs met. This transcends healthcare and encroaches on virtually every part of life. Adapting her new home to suit Kieran’s changing requirements involved local planners, architects, occupational therapists, builders and an NHS review panel. The process took two years, during which time the family “survived in a house that was totally unsuitable”.

Kieran needs nine pieces of equipment, including a ventilator, switched on 24 hours a day at home to keep him alive and looked after. This year, Louise estimates she will need to find an additional two-to-three thousand pounds for energy costs.
Many of Dr Shah’s patients are in similar positions. He said: “They’re already more deprived than other people and now the energy crisis is going to hit them even more because they use energy more than we do. That’s a very acute problem.”
COVID-19 has both exposed and exacerbated problems. When COVID-19 hit, Kieran’s carer was no longer able to visit their home, so responsibility fell to Louise and her other son, Harvey, who left his job. A three-day hospital stay for a procedure became three months when Kieran’s ward was turned into a COVID-19 ward. He returned a different person, Louise said, after being without her for so long. It’s worse now things are opening back up, Louise said: “As the rules have decreased, we have increased ours. I'm now finding people are starting to treat me like I'm slightly deranged if I ask them to put on a mask.”
While most societal problems are beyond the means of the healthcare profession alone to solve, there is some evidence that healthcare itself could be exacerbating issues. Analysis published last month in the British Medical Journal (BMJ), co-authored by Dr Akanksha Mimi Malhotra, Vice- President of the Royal Society of Medicine Respiratory Medicine Section, suggests that healthcare may be less safe for some patients than for others. For example, research shows that ethnic minority patients are at increased risk of hospital-acquired infection, adverse drug effects and pressure ulcers. Similarly, people who are socioeconomically disadvantaged and those with learning disabilities are more likely to experience delayed healthcare intervention. The authors assert that we have “an opportunity to deliver meaningful change” and call for co-ordinated action to address healthcare biases. In recognising these risks, healthcare professionals can work to mitigate them in their care of specific patient groups.
Such systemic changes will take time and require an unprecedented level of co-ordination between the NHS, government and other bodies.
Part of the reason health inequalities are so entrenched and intractable is that they can be self-perpetuating. Inequality often causes poor health and poor health often causes inequality.
Some solutions, such as more targeted investment in smoking cessation, promoting healthy eating, encouraging less-sedentary lifestyles and educating about air pollution and the benefits of vaccines, are relatively easy to prescribe but less simple to deliver. The answer is not necessarily more money but being smarter about how it is spent and including patients in those conversations, suggests Dr Shah.
If the pandemic has taught us anything, it is that co-ordinated impacts on a major scale are possible when we are facing an acute crisis. The question now is whether we can collectively channel similar energy into chronic, but equally destructive, issues. If we can, the legacy of the past two years could, paradoxically, be better and fairer healthcare for all.
The Royal Society of Medicine has recently launched a major multi-year programme to tackle health inequalities, opening with a flagship conference in Autumn 2022 in partnership with NHS England and NHS Improvement.
This is the first in a series of features in support of the RSM’s Tackling Inequalities programme. Each examines health inequalities through the lens of a different RSM section. This article focused on respiratory medicine. Thank you to all contributors.
You can join the conversation on social media using the hashtag #tacklinginequalities. If you have a suggestion for a future feature or wish to contribute, please email [email protected].